Burns are the most common injury received at home or at work. In case of burns, it is important to properly provide first aid and consult a doctor. The most common origin of this injury in everyday life is getting burned with boiling water. Unfortunately, treatment of burns it has become overgrown with serious myths, because of which first aid is wrong.
By treatment of burns it is extremely important to choose effective anesthesia and stimulate the repair processes. TES therapy stimulates reparative-regenerative processes in a burn wound, which is accompanied by an improvement in the general condition of patients, early elimination of symptoms of intoxication, normalization of sleep, appetite, and a decrease in the severity of pain syndrome.
When using TES therapy, the treatment time for burn victims is significantly reduced compared to traditional methods. In addition, with the help of the transcranial pulse bipolar electrostimulator “DOCTOR TES-03”, it is possible treatment of burns at home, if the degree of the burn does not provide for hospitalization and a doctor has been consulted.
Attention! Treatment of burns of any degree, including burns with boiling water – treat only under the supervision of a doctor! Home treatment of burns only after consulting a doctor! Treatment of burns is serious! Be attentive to your health!
THE EFFECTIVENESS OF TRANSCRANIAL ELECTRICAL STIMULATION IN THE TREATMENT OF PATIENTS WITH BURNS
GERASIMOVA L. I., KONDRIKOVA E. S., GRISHCHENKO A.V., KAREV V. A., PUTINTSEV A. N.
Department of Acute thermal lesions of the Institute of Emergency Medicine. N. V. Sklifosovsky,
Information Technology Department of the N.N.Priorov Central Institute of Traumatology and Orthopedics, Moscow
Transcranial electrical stimulation (TES) is a method of electrotherapy in which selective activation of central regulatory systems (hypothalamic—pituitary-adrenal, opioid, etc.) is achieved by exposure to a specially selected weak electrical signal on the median structures of the brain. The TPP method, developed in our country by Professor V.P.Lebedev [1, 2, 3], is used in the clinic to relieve stress and accelerate the course of reparative processes in the treatment of patients with myocardial infarction [4, 5], diseases of the nervous system [6, 7], gastric ulcer and duodenal ulcer [8] and other pathological conditions.
For the first time for the treatment of patients with burns, the TES method was used in the department of acute thermal lesions of the Institute of Emergency Medicine. N. V. Sklifosovsky in 1987, Professor L. I. Gerasimova and Cand. biol. sciences E. S. Kondrikova. The encouraging results obtained made it possible to continue research in patients with various severity of burns, including mass and group admissions of victims from the foci of domestic and man-made disasters.
Indications for the choice of the TES method were determined based on the assessment of the severity of the systemic reaction of the body to a burn injury, the premorbid status of the patient and the local tissue reaction. In this regard, TES was used in patients with varying severity of burns while maintaining severe pain syndrome and other manifestations of acute and chronic stress, maladaptation and inflammation in wounds that developed as a result of the injury.
MATERIAL AND METHODS
Studies were conducted in 207 patients with burns of II—III— IV degree on an area of 5-80% of the body surface (pt), of which the area of deep burns was 2-40% pt, of which 105 patients received TES, and 102 patients adequate in severity of the burn, age and gender, treated with traditional methods, made up the control group group (Table 1).
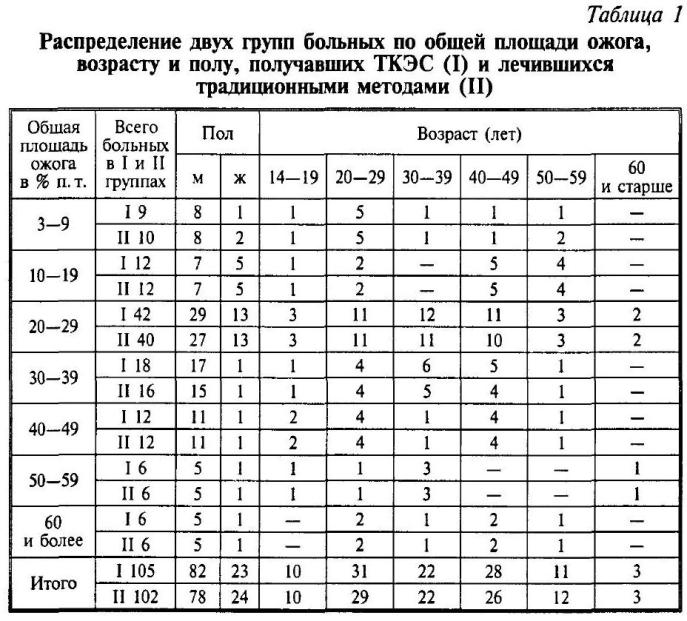
Table 1 shows that among the examined patients, men of working age prevailed with lesions of more than 10% p. t. Patients of the main and control groups were comparable in total burn area, age and gender.
Among 86 patients, TES treatment was started within the first 2-4 days after the injury, in the remaining 19 — on the 3rd-10th day. TPP sessions were performed on domestic Transair-2, MDM-1, MDM-101 and MDM-3 devices approved for use in medical practice. The location of the electrodes is frontal-mastoid or frontal-occipital, the pulse current frequency is 77-80 Hz (Transair-2 and MDM-1 devices) or variable from 60 to 90 Hz (MDM-101, MDM-3 devices).
The shape of the pulsed current is rectangular (Transair-2, MDM-1, MDM-101 and MDM-3) or pointed-two-phase (MDM-3). The ratio of constant and variable components is 1:1. The current strength was set in the range of 0.5— 2.5 mA (when using rectangular pulses) and 1.0—6.0 mA (with pointed-two-phase pulses) individually until the appearance of specific sensations of “tingling” or “light burning” under the electrodes.
The course of treatment in 21 patients with grade II superficial burns up to 20% p. t. was 5-10 daily sessions, the 1st session – 20 min., all subsequent — 30 min. with a break for 1 day, but not earlier than after the 4th session. The course of treatment of 84 patients was 8-15 daily sessions of 30 minutes with breaks of 1 day after the 4th and 8th sessions, if TES was used for more than 10 days. In 8 of these patients, TES sessions were conducted 2 times a day for 15-20 minutes.
The treatment of patients with thermal power plants, as well as patients of the control group, was carried out against the background of complex intensive therapy and active surgical tactics developed in the department of acute burn lesions.
The effectiveness of TES was evaluated according to clinical data: reduction or elimination of pain syndrome, normalization of sleep, appetite, decrease in the severity of depression and negative attitude to treatment. The patients also independently assessed the change in their condition before and after the TES course as a percentage of the initial one.
The pulse (PS), the frequency of respiratory excursions of the chest (BH), central (Tc) and peripheral (Tp) temperatures were recorded on a Brucer monitor (Germany), the temperature gradient (Tc-Tp) was calculated. Content ?-endorphin and somatotropic hormone were determined by radioimmunological methods (studies were performed in the radioimmunological laboratory of the Institute of Experimental Cardiology of the Russian Academy of Medical Sciences, Head of the laboratory Professor Yarygin V. K.). Calculations and statistical data processing were carried out by the Student’s method. The reliability of the changes in some cases was determined by the analysis of paired changes calculated in percentages (— M%).
RESULTS AND THEIR DISCUSSION
Observations have shown that the TES method is well tolerated by patients with burns of varying severity, regardless of age and gender, and does not cause any adverse reactions and complications. During the treatment of thermal power plants, the threshold of current tolerance increases until the appearance of specific sensations of “tingling” or “light burning” under the electrodes.
When using rectangular pulses, this increase is 20-80% of the initial value (on average 36 +11); with pointed-two—phase pulses – 200-400% (on average 356 ± 86) with a noticeable increase already during the second TPP session. It can be assumed that the pointed-two-phase pulse signals of thermal power plants are better tolerated by burn patients.
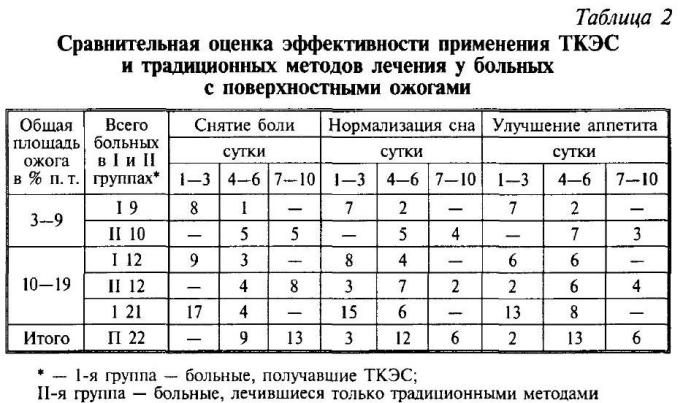
In the course of treatment of patients with superficial burns up to 20% p. t. (Table. 2) pain reduction by the end of 3 days occurred in 17 of the 21 patients receiving TES, while in all patients of the control group, pain persisted. At the same time, sleep returned to normal in 15 patients who received TES and only in 3 treated with traditional methods, and in 6 patients of the control group, sleep disorders were observed even after a week’s stay in the department. Improvement of appetite in the first 3 days was noted in 13 patients receiving TES and in 2 from the control group.
When analyzing laboratory parameters in patients treated with TES, normalization of the Arent formula on the 6th-7th day was noted in the peripheral blood due to a decrease in the rod-nuclear shift from 11 to 5% (p < 0.05), an increase in the content of lymphocytes from 8 to 21% (P<0.05) and the elimination of toxic neutrophil granularity, whereas in patients of the control group, these indicators returned to normal later — on the 9th-10th day. The initial level of average molecules in blood plasma in patients of the main and control groups was almost the same and ranged from 0.376 to 0.308 units, indicating moderate signs of intoxication.
During the treatment of thermal power plants by the 7th day after injury, the content of average molecules in blood plasma decreased on average from 0.346 to 0.243 units (p < 0.05), and in patients of the control group their level remained elevated – 0.312—0.303 units and decreased to 0.252 units only by the time of discharge from the hospital. There were no significant changes in urine in patients of both groups, and short-term proteinuria in the first days after the injury was eliminated by the end of the 1st week.
Increase in content ?-endorphin in blood plasma on average from 56.6 to 93.3 pG/ml (p < 0.05) was in 15 patients studied before and after the completion of the TES course. However, 5 of them had a decrease in the level after the first TPP session?-endorphin up to 36.7—42.3 pG/ml. In subsequent sessions , the content ?-their endorphin increased and steadily exceeded the initial level. The content of somatotropic hormone in the blood increased after a course of TES treatment from an average of 0.88 to 1.24 nG/ml (p < 0.05) in 15 patients. In the control group , the initial content ?-endorphin and somatotropic hormone were lowered, respectively, 54.9 pG/ml and 0.91 nG/ml, and did not change significantly at the end of treatment.
In the course of treatment of patients with extensive burns, it was noted that the elimination of pain syndrome, normalization of sleep and improvement of appetite in patients receiving TES allowed to cancel the use of painkillers, hypnotics and sedatives after the 3rd-4th session, whereas in the control group these drugs continued to be used as pathogenetic treatment (Table 3).
Against the background of TPP, the wound process proceeded smoothly, there were no general and local complications, the average time of hospitalization averaged 15 days, and in the control group — 18. These data show that in patients with extensive burns of II—III—IV degrees who received TES, pain relief, sleep normalization and relief of hyporexia were achieved much sooner than in patients treated with traditional methods. 51 of the 61 studied patients (on average 60.5±8.2%) and 10 – by 35-45% (on average 38.6±3.6%) noted an improvement in their condition during the course of TES treatment by 50-70% from the baseline.
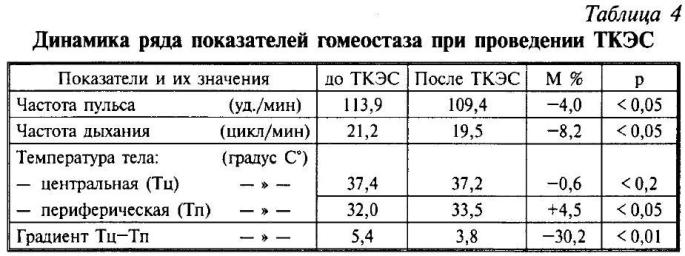
Evaluation of the studied indicators of homeostasis in patients receiving TES (Table. 4), revealed a decrease in tachycardia and respiratory rate, an increase in peripheral temperature and a decrease in temperature gradient. The normalizing effect of TPP was the stronger, the more pronounced the previous shifts in these indicators of homeostasis were.

The initial content of beta-endorphin and somatotropic hormone in the main and control groups on the 3rd-10th day (Fig. 1) averaged 62.6 pG/ml (norm 60-120 pG/ml) and 0.81 nG/ml (norm 1.2—1.4 nG/ml), respectively.
Upon completion of the TES course, 25 patients showed a persistent increase in the content of beta-endorphin in blood plasma to an average of 101.8 pG/ml (p<0.05) and somatotropic hormone to an average of 1.85 nG/ml (p<0.05). In 7 patients, after the first session, a decrease in beta-endorphin in plasma was observed to 39.3-45.6 pG/ml, which increased to 88.3—98.1 pG/ml during subsequent TES sessions and steadily exceeded the baseline level. Apparently, these patients had insufficient adaptive response after the first TES session.
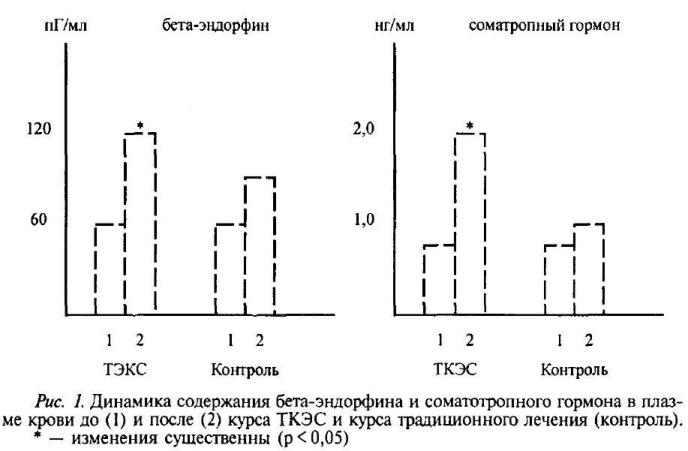
Among 22 patients of the control group, the content of beta-endorphin and somatotropic hormone did not change significantly during treatment, it was kept at the lower limit of the norm, respectively 62.6-76.2 pG/ml and 0.81—1.03 nG/ml.
The elimination of pain syndrome, normalization of sleep and improvement of appetite in 72 out of 84 patients (85%) who received TES made it possible to almost completely eliminate the use of painkillers, hypnotics and sedatives after the 3rd-4th session and in patients with extensive deep burns, while these funds continued to be used in the treatment of patients of the control group.
Our research and literature data indicate that the mechanism of action of TES involves stimulation of the opioid system (in particular beta-endorphin) and the production of pituitary hormones (in particular somatotropic hormone). In our opinion, generalized changes in the multilateral correlation of neuroendocrine regulatory structures appear in patients with burns under the influence of thermal power plants, leading to activation of a sufficiently strong adaptation simultaneously with an antistress effect.
This makes the TES method indicated in the treatment of patients with both limited and extensive surface and deep burns with signs of acute or chronic stress and maladaptation.
The presence of correspondences in the results of clinical and laboratory studies, in our opinion, indicates the combined nature of the changes caused by TES, since the processes of subordination, subordination and reciprocal distribution of the level of functional state are inevitable in the systemic reaction of constantly working brain centers.
In accordance with these and previous studies [9, 10, 11, 12, 13] we believe that activation of the antinociceptive system leads to improvement of microcirculation, metabolism and sertonin metabolism, alignment of reactions and feedback between central regulatory mechanisms, organs and systems. The manifestations of the systemic reaction in this case are modulating in nature with the achievement of normalization of the processes of inhibition and excitation, the appearance of adequate rest and toning effect.
In the mechanism of action of thermal power plants, it is important to reduce hypoxia and normalize appetite in patients with burns, directly related to improving the secretion of digestive glands, the suction and motor function of the gastrointestinal tract. These manifestations of the general adaptation syndrome are reflected in the subsequent anti-inflammatory and biostimulating action [14, 15].
When assessing the effect of thermal power plants, it can also be assumed that one of the main causes of violations of the regulatory functions of nerve structures in burned patients is a shortage of electrons necessary for the formation of nerve impulses in the wound itself and the adjacent areas.
Consequently, the modulating effect of the process of redistribution of electrons from nerve structures with their excessive content into structures depleted of electrons and partially or completely lost the ability to regenerate their controlling or controlling nerve impulses is likely to be the basis of the mechanism of action of the thermal power plant.
These assumptions were confirmed by the consistent use of thermal power plants and magnetic laser therapy (MLT) in burned patients, which provided relief of pain syndrome and increased reparative-regenerative processes in burn wounds in those patients in whom the isolated use of both methods did not create the expected effect [16].
Currently, the research materials on the use of thermal power plants as a new method of electrotherapy are presented in the monograph “Thermal and radiation burns” [17] and they are a fragment of the information and reference system “Burns” [18], designed to quickly obtain the necessary information on the organization and provision of optimal assistance to victims with thermal trauma.
Thus, the scientific and practical significance of our considerations on the mechanism of action of thermal power plants indicates the versatility of physiological effects occurring in the body of patients with burns, and can serve as a support for the doctor in determining indications, contraindications and choosing tactics for the use of this method of electrotherapy together with magnetolaser therapy in the treatment of patients with burns, including their mass or group admissions to specialized centers after domestic or man-made disasters.
Conclusions:
1. The TES method is well tolerated by patients with varying severity of burns and does not cause any adverse reactions and complications.
2. The indication for the use of thermal power plants in patients with burns is the presence of manifestations of acute or chronic stress and maladaptation.
3. The use of TES reduces and then relieves pain syndrome, normalizes sleep and appetite, modulates the content of beta-endorphin, sosomatotropic hormone in blood plasma and manifestations of a systemic reaction to burn injury, stimulates the reparative process.
4. Consistent application of TES and MLT allows overcoming antinociceptive stimuli from the periphery and restoring the modulating influence of regulatory centers on reparative-regenerative processes in burn wounds in cases of lack of effect with isolated use of these methods.
5. The mechanism of action of TES is complex and, including changes in the activity of opiate mechanisms in the structures of the antinociceptive system, ensures the achievement of an antistress effect and increased adaptation in patients with burns.
literature
1. Lebedev V.P., Katsnelson Ya.S, Leosko V.A. et al. — Method of general anesthesia. — A. S. No. 1054543, 1983
2. Lebedev V. P. — Directed activation of opioid systems of the brain stem: analgesic and conjugate effects. — Tez. All-Union. conf. “Experimental and clinical pharmacology of painkillers”. L., 1986, 90-92.
3. Lebedev V. P. — Transcranial electroanalgesia.— Collection of materials “A new method of drug-free treatment”. St. Petersburg, 1993, 9-17.
4. Golikov A. P., Ryabinin V. A., Lebedev V. P. et al . — A method of treating patients with acute myocardial infarction. A. S. No. 1507404, 1989
5. Pavlov V.A. — The effect of transcranial electrical stimulation on opioid systems and the course of myocardial infarction. — Abstract of diss. cand. med. sciences’. M., 1989, — 20 p.
6. Akimov G. A., Volkov A. K. — The experience of using transcranial electrical action in the treatment of diseases of the nervous system. — Sat. materials “A new method of drug-free treatment”, St. Petersburg, 1993, 69-70.
7. Voitenko R.I., Kokin G. S., Lebedev V. P., Tyshkevich T. G. — Transcranial electroanalgesia in the treatment of pain syndrome in peripheral nerve injuries. — Sat.